

Thrombus is the principle discovering in most sufferers with acute coronary syndrome (ACS), the kind of which doubtlessly impacts the tip results of the interventional process by way of no reflow and edge dissection. Optical coherence tomography (OCT) is taken into account a exact intra-vascular software to picture thrombi and characterise its properties. We aimed to check the influence of thrombus kind, as outlined by OCT, on procedural end result in ACS sufferers. On this retrospective research we enrolled 100 sufferers who have been handled by percutaneous coronary intervention (PCI) with the steerage of OCT. We recorded demographic and medical knowledge of the entire studied cohort. Angiographic particulars and procedural knowledge have been famous. Baseline OCT research was carried out earlier than intervention and repeated post-intervention. Plaque characterisation was recognized, and thrombi have been outlined as purple or white thrombi. Acute angiographic end result was outlined with particular emphasis on no reflow.
Male sufferers and ST-elevation myocardial infarction (STEMI) sufferers extra usually had white thrombi (58.1% and 71.2%, respectively). Instances with purple thrombi had longer ache length, which was statistically vital. Edge dissection was extra frequent with purple thrombus, 44.7% versus 32.1% with white thrombus, however the distinction is just not statistically vital, whereas 17% of sufferers with white thrombi have been sophisticated by no-reflow phenomenon versus solely 4.3% in sufferers with purple thrombi, and this distinction was statistically vital.
In conculsion, OCT-guided PCI is possible and protected in ACS settings. OCT-guided intra-procedural differentiation of thrombus kind is doubtlessly helpful in predicting acute procedural end result.
Introduction
Acute coronary occasions are generally brought on by plaque rupture, erosion and, sometimes, calcific nodules. Within the majority of sufferers with acute coronary syndrome (ACS), occlusive or sub-occlusive thrombus on high of plaque deformation is the principle angiographic discovering. Resolving acute thrombotic occlusion stays the cornerstone step in restoring ample coronary perfusion. Blind coping with thrombi, relying solely on angiography, could also be an impediment to optimum myocardial perfusion and improve in-hospital morbidity and mortality.1–4
Up to now, intravascular ultrasound (IVUS) and, extra not too long ago, optical coherence tomography (OCT) have been regularly used for percutaneous coronary intervention (PCI) optimisation. Pre-PCI intra-vascular imaging, paved the way in which to exactly assess lesion significance, plaque options, necessity of lesion preparation and correct stent selection relating to width and size.4–6
Frequency area OCT, as in contrast with IVUS, has 10 instances higher axial decision, weak penetration functionality (1–2 mm) and requires clearance of luminal blood. IVUS utilises ultrasound waves, in distinction to OCT, which is dependent upon infrared mild with minimal wavelength (1–3 µm) yielding magnificently larger decision, however with out passable tissue penetration. The wavelength of purple blood corpuscle is far better than OCT wavelength, so backscattering happens if luminal blood is just not cleared first, earlier than beginning pullback. The mixture of tremendous decision with minimal penetration permits easy distinction between plaque and abluminal floor, selling OCT to be extra superior in luminal measurements and clarifying thrombus composition.5–7
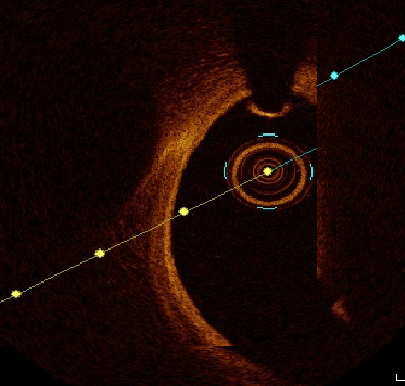
Frequency-domain OCT provides the privilege of going by way of the pathophysiology of unstable plaque, to distinguish between plaque rupture and erosion. Thrombi have been outlined as protrusions into the vessel lumen, and characterised in line with their sign traits. White thrombus was recognized as a signal-rich, low-backscattering thrombus, whereas purple thrombus was recognized as high-backscattering protrusions, with signal-free shadowing.8–14
PCI success may be hindered by the presence of intra-coronary thrombi, which influences acute procedural success by way of enhancing coronary movement, thrombus prolapse and distal edge dissection. Influence of thrombus morphology and histology on procedural end result has not been clearly studied. Relying on the bodily traits of OCT, it’s the most anticipated to exactly make clear thrombus kind and research its influence on end result.
We aimed to check the influence of thrombus kind as outlined by OCT on procedural end result in ACS sufferers.
Methodology
Between January and June 2022, 760 circumstances of myocardial infarction have been admitted to our centre, an invasive technique together with major PCI was adopted in 524 sufferers. Of those, 131 sufferers underwent OCT-guided interventions primarily based on operator expertise and availability of probes; nonetheless, 31 sufferers have been excluded both on account of inappropriate picture acquisition or on account of extreme percutaneous transluminal coronary angioplasty (PTCA) with potential thrombus deformation. The remaining 100 sufferers met our inclusion standards and have been enrolled retrospectively. The exclusion standards have been: end-stage nephropathy, post-coronary artery bypass graft (CABG) sufferers, poor OCT picture and sufferers with completely occlusive thrombi, even after wiring and thrombus aspiration. Written consent was achieved from each affected person earlier than participation.
Examine inhabitants
Full historical past taking and exact medical examination have been finished for all topics. ST-elevation myocardial infarction (STEMI) was outlined as typical chest ache for half-hour a minimum of, arrival to centre with major PCI services inside 24 hours from onset of chest ache, ST-segment elevation >0.1 mV in two or extra contiguous leads or newly detected left bundle-branch block. Non-ST-elevation myocardial infarction (NSTEMI) was outlined as extended chest ache with optimistic cardiac biomarkers with out ST-segment elevation. We outlined the perpetrator vessel by electrocardiogram (ECG) standards, or throughout angiogram as thrombus-containing vessel.13
Throughout hospital course, serum creatinine was serially withdrawn. Period of hospital course was recorded and early post-PCI adverse outcomes have been talked about. Sufferers have been adopted in outpatient clinic for six months to detect main opposed cardiovascular occasions (MACE).
Affected person preparation and OCT process
Antithrombotics have been administered matching the most recent common pointers. Drug-eluting stents have been deployed. Lesion measurements have been finished in two orthogonal views and end-diastolic frames have been chosen, after giving a minimum of 200 µg of nitrates. Put up-OCT research, thrombotic lesions have been categorised in line with thrombus kind into white and purple thrombi.
A extensively used frequency area OCT system (Ilumien System, Inc., St. Jude Medical, USA) and a 0.014 inch wire (Picture Wire, St. Jude Medical, USA) have been used. Motorised wire pull-back at 10 mm/s was finished throughout distinction injection. OCT measurements have been mentored by an OCT specialist.2,15
Plaque morphology was outlined by way of each body; plaque rupture was outlined as discontinuity of the fibrous capsule with plaque cavitary formations. Plaque erosion was outlined as irregular lumen with thrombosis overlying intact cap. Thrombus was categorised to purple and white thrombi in line with composition, attenuation diploma and backscattering. White thrombus was outlined as a signal-rich, low-backscattering mass, whereas purple thrombus was outlined as high-backscattering protrusions contained in the lumen, with signal-free shadowing as proven in figures 1 and a couple of.2,16,17
The OCT evaluation included luminal areas on the proximal and distal referenced segments, minimal lumen areas (MLA), minimal stent space (MSA). MSA exceeding 90% was thought-about optimum and ≥80% was acceptable. Dissection was outlined as disruption of luminal intimal floor on the stent edges, and tissue prolapse was outlined as protrusion of tissue by way of stent struts. Thrombolysis in Myocardial Infarction (TIMI) movement grade was recorded with particular emphasis on incidence of no reflow.11–14,18
No reflow is outlined as insufficient tissue perfusion by way of a given phase of the coronary circulation with out angiographic proof of main vessel obstruction.19
The administration protocol of no-reflow phenomenon was primarily pharmacological by way of the intra-coronary injection of glycoprotein IIb/IIIa inhibitors, verapamil, sodium nitroprusside, adenosine and, sometimes, epinephrine.20
It’s price mentioning that thrombus identification by OCT is very subjective and operator dependent.21
Statistical evaluation
Statistical testing was finished utilizing the Statistical Bundle for Social Sciences (SPSS) model 20. Steady variables have been introduced as imply ± normal deviation (SD). Categorical variables have been introduced as numbers and percentages. Kolmogorov-Smirnov take a look at for regular distribution was used to delineate between parametric and non-parametric knowledge. Evaluation of variance (ANOVA) take a look at was used to evaluate relations between totally different variables. Univariate and multi-variate evaluation was finished. For all assessments, a p worth lower than 0.05 was thought-about a major distinction.
Outcomes
Demographic knowledge and threat elements
Desk 1. Demographics and threat profile
N=100
Quantity
%
Male genderFemale gender
8614
8614
People who smoke
79
79
Hypertension
60
60
Diabetes mellitus
34
34
Hyperlipidaemia
48
48
Peripheral vascular illness
0
0
Cerebrovascular accident
6
6
Earlier MI
7
7
Earlier PCI
23
23
Imply ± SD
Vary
Age, years
53.3 ± 11.3
28–85
Period of signs, hours
9.7 ± 8.6
2–48
Key: MI = myocardial infarction; PCI = percutaneous coronary intervention; SD = normal deviation
100 sufferers have been enrolled on this research. Sufferers’ demographic and medical knowledge are summarised in desk 1. The imply age of studied sufferers was 53.3 years with males representing 86% of the studied cohort. Imply length of chest ache was 9.7 hours. Probably the most encountered threat elements have been: cigarette smoking (79%), hypertension (60%), hyperlipidaemia (48%) and diabetes (34%), respectively. Six topics had beforehand skilled cerebrovascular stroke.
Wrongdoer lesion traits
Many of the sufferers on this research have been STEMI sufferers (66%), two sufferers had acute pulmonary oedema and one affected person was in cardiogenic shock. Of perpetrator lesions, 67% confirmed plaque rupture versus 33% with plaque erosion. Wrongdoer vessel confirmed white thrombus in 53 topics whereas 47 sufferers had purple thrombus. No reflow was managed efficiently utilizing intra-coronary drugs in 11 sufferers. Wrongdoer lesion options are proven in desk 2.
Procedural end result
Drug-eluting stents have been implanted in all topics. Wrongdoer vessel was left anterior descending (LAD) 73%, proper coronary artery (RCA) 18%, left circumflex (LCx) 10%, left essential trunk 3%, and diagonal 3%. OCT research post-intervention revealed imply stent growth of 93.2% and imply MSA of 8 mm2. Limiting edge dissection was detected in six sufferers, tissue prolapse encountered in 38 circumstances and related mal-apposition necessitating optimisation in 56 sufferers (desk 3).
Desk 2. Wrongdoer lesion morphology by optical coherence tomography (OCT)
N=100
Quantity
%
95percentCI
STEMI casesNSTEMI circumstances
6634
6634
55 to 75percent24 to 44%
No-reflow phenomenon
11
11
5 to 18%
Plaque rupture group
67
67
56 to 76%
Plaque erosion group
33
33
23 to 43%
Fibrous plaque
24
24
Calcific plaque
12
12
Necrotic fibrous plaque
64
64
Thrombus kind
Purple thrombi
47
47
36 to 57%
White thrombi
53
53
42 to 63%
Imply ± SD
Vary
Reference vessel diameter, mm
3.3 ± 0.5
2.2–4.7
Lesion dimensions, mm
1.52 ± 0.3
0.9–3
MLA in mm2
2.65 ± 1.0
0.8–8
Key: CI = confidence interval; MLA = minimal luminal área; NSTEMI = non-ST-elevation myocardial infarction; SD = normal deviation; STEMI = ST-elevation myocardial infarction
Desk 3. OCT research post-intervention
N=100
Quantity
%
Edge dissection
6
6
Tissue prolapse
38
38
Important mal-apposition
56
56
Imply ± SD
Vary
Stent growth, %
93.2 ± 4.5
86–114
Ultimate MSA, mm2
8.0 ± 2.7
3.7–15.8
Key: MSA = minimal stent space; SD = normal deviation
White thrombus versus purple thrombus
The studied cohort was categorised in line with thrombus kind to 2 teams: white thrombus (53%) versus purple thrombus (47%). Each teams have been in contrast in line with demographic and medical knowledge as proven in desk 4. White thrombus was discovered to be considerably extra evident (58.1%) amongst male sufferers (p=0.009). Youthful age at presentation was considerably associated to white thrombi, whereas people who smoke solely confirmed a pattern for that. There isn’t any statistically related distinction relating to thrombus kind amongst hypertensive, diabetic, or dyslipidaemia sufferers. White thrombi have been considerably evident in STEMI sufferers (71.2%, p=0.000 with odds ratio 11.5) whereas in NSTEMI sufferers, white thrombi represented a minority. Instances with purple thrombi had longer ache length earlier than presentation as in contrast with white thrombi, which was vital statistically (13.7 ± 9.4 vs. 6 ± 4.6 hours) as proven in desk 4.
Desk 4. Comparability between demographic and medical variables as regards thrombus kind
Purple thrombusNumber (%)
White thrombusNumber (%)
p worth
Male gender N=86
36 (41.9)
50 (58.1)
0.009
Younger (<55.3 years) N=50
17 (34)
33 (66)
0.009
Smoker N=79
33 (41.8)
46 (58.2)
0.04
Hypertensive N=60
32 (53.3)
28 (46.7)
0.1
Diabetic N=34
18 (52.9)
16 (47.1)
0.3
Dyslipidaemic N=48
26 (54.2)
22 (45.8)
0.1
STEMI N=66
19 (28.8)
47 (71.2)
NSTEMI N=34
28 (82.4)
6 (17.6)
0.000
Purple thrombusMean ± SD
White thrombusMean ± SD
Ache time in hours
13.7 ± 9.4
6 ± 4.6
0.000
Key: NSTEMI = non-ST-elevation myocardial infarction; SD = normal deviation; STEMI = ST-elevation myocardial infarction
Composite adverse procedural end result in relation to thrombus kind
Thrombus prolapse reveals no statistically vital distinction between each kinds of thrombi. Edge dissection was observed extra regularly with purple thrombus 44.7% versus 32.1% amongst circumstances with white thrombus and the distinction is just not statistically vital. No-reflow phenomenon sophisticated 17% of sufferers with white thrombi versus solely 4.3% of sufferers with purple thrombi, and this distinction was statistically vital. Collectively, the next proportion of mixed adverse outcomes was witnessed amongst circumstances of purple thrombi, however with no statistical significance (desk 5).
Desk 5. Comparability between kind of thrombus as regards adverse outcomes detected by OCT
Purple thrombusNumber (%)
White thrombusNumber (%)
p worth
Prolapse
3 (6.4)
3 (5.7)
0.8
Dissection
21 (44.7)
17 (32.1)
0.1
No reflow
2 (4.3)
9 (17)
0.04
Mixed adverse end result
23 (48.9)
23 (43.3)
0.5
Desk 6. Logistic-regression mannequin of thrombus kind and the no-reflow phenomenon as a adverse end result throughout intervention
No reflow
Wald
p
Exp(B)
95percentCI
Thrombus kind(Purple as having threat)
0.22
0.05 to 1.1
3.5
0.059
p>0.05 not significantKey: CI = confidence interval
Confirming the earlier knowledge in desk 5, a logistic-regression mannequin was carried out supporting that no reflow was not statistically associated to purple thrombi as in contrast with white thrombi with an odds ratio of 0.22, as proven in desk 6.
Six-month follow-up
Recruited topics have been adopted for six months in outpatient departments, no MACE have been encountered by way of cardiovascular-related mortality, myocardial infarction or goal vessel re-intervention, other than minor bleeding in a single topic and two sufferers’ admission with decompensated coronary heart failure.
Dialogue
The important goal of this research was to test the feasibility of OCT steerage in differentiating purple and white thrombi inside perpetrator lesions of ACS, thereafter, which kind is extra associated to adverse procedural outcomes similar to no reflow, edge dissection, thrombus prolapse and their mixed finish level.
Many of the ACS sufferers in our research have been presenting with STEMI (n=66). Plaque rupture was encountered in 77% of sufferers, the place it represented 83% of STEMI circumstances, whereas plaque erosion represented 64% of NSTEMI sufferers. This discovering is taken into account a rehearsal of what Guagliumi et al., Fang et al., and Dai et al. discovered of their research.22–24
Earlier than discussing our focused differentiation of thrombus sorts to purple and white, a vital clarification must be finished, due to which a whole lot of ACS sufferers weren’t recruited to our research. OCT-guided thrombus and plaque evaluation was finished provided that a minimum of TIMI movement ≥2 was achieved after perpetrator lesion wiring ± thrombus aspiration, however not after PTCA, fearing that PTCA might alter plaque morphology or add to adverse outcomes as no reflow earlier than our evaluation. This pathway was additionally finished by Amabile et al. once they studied thrombus burden by OCT earlier than and after deferral of PCI in STEMI sufferers in 2014.25
White thrombus was extra evident in male gender (58.1%) and likewise in younger age (<53 years, our imply age) whereas people who smoke solely trended for that. This may be attributed to early time of presentation in younger male smoker sufferers who aren’t preconditioned to ischaemia on the time of presentation, when the thrombus is principally shaped of platelets, earlier than fibrin meshwork is properly established and purple blood cells profoundly settle within the clot. Different atherosclerotic threat elements similar to hypertension, diabetes or dyslipidaemia weren’t statistically totally different between the 2 kinds of thrombi.
White thrombi have been constantly current in STEMI sufferers (71.2% of STEMI sufferers) however they represented a minority in NSTEMI sufferers, whereas the reverse was encountered with purple thrombi. The group of sufferers with purple thrombi had an extended length of ache earlier than presentation (13.7 ± 9.4 hours) in contrast with the group with white thrombi (6 ± 4.6 hours), which can be a dart to our level that fibrin mesh maturation and purple blood cell settlement current after an extended time.
Regardless of a paucity of knowledge about thrombus kind in relation to totally different demographic, medical and angiographic displays, shades of our knowledge have been echoed in a overview of literature revealed by Khandkar et al. in 2021 concerning the mechanistic variations amongst ACS sufferers, find out how to detect by imaging (the place OCT absolutely was advisable as the perfect) and the way this will have an effect on the focused process plan.26
As for acute procedural adverse outcomes, our research centered on no reflow, thrombus prolapse and dissection. White thrombi have been discovered to be strongly associated to incidence of no reflow, which occurred in 17% of white thrombi sufferers versus solely 4.3% of purple thrombi sufferers. Once more, this was not said as solidly as we state earlier than, however urged by Khandkar et al. by relating ruptured fibrous cap to STEMI sufferers to white thrombi, then relating no reflow to STEMI sufferers.26
Logically, if no-reflow phenomenon is usually on account of micro-thrombi dislodgement to distal circulation after PTCA or stent deployment, as said in virtually all literature discussing this phenomenon, this shall occur extra generally with the platelet-rich white thrombi than with the fibrin and purple blood cell-rich purple thrombi. This might additionally clarify the nice response of no reflow to intracoronary glycoprotein IIb/IIIa inhibitors to cease platelet aggregation and white thrombus propagation.20,22
Concerning thrombus prolapse, there was no vital distinction between the 2 kinds of thrombi, whereas dissection was encountered extra with purple thrombi sufferers however with out statistical significance. Additionally, the mixed adverse end result confirmed no distinction between the 2 thrombi sorts.
This research is just not a limitation-free research, being a non-randomised research, choice bias and different types of bias can’t be excluded. Furthermore, the research was not empowered to detect variations in MACE or different medical outcomes. So, bigger randomised medical research are wanted to make clear these gaps of proof. Regardless of these limitations, we do imagine that our knowledge are doubtlessly including to the physique of proof supporting using OCT as the perfect intra-vascular imaging modality to optimise acute procedural outcomes in ACS sufferers.
Conclusion
OCT-guided PCI is possible and protected amongst sufferers with ACS. OCT-guided intra-procedural differentiation of thrombus kind is doubtlessly helpful in predicting acute procedural end result.
Key messages
Optical coherence tomography (OCT) is possible in setting of acute coronary syndrome (ACS) when utilized by skilled fingers
OCT can completely optimise angiographic end result post-percutaneous coronary intervention (PCI)
White thrombus is a serious threat issue of no reflow
Anticipation of no reflow is feasible with intravascular imaging
Conflicts of curiosity
None declared.
Funding
None.
Examine approval
The research had moral approval quantity FMASU R 162 2022.
References
1. Virmani R, Burke AP, Kolodgie FD et al. Classes from sudden coronary loss of life: a complete morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol 2000;20:1262–75. https://doi.org/10.1161/01.ATV.20.5.1262
2. Jia H, Aguirre AD, Abtahian F et al. In vivo analysis of plaque erosion and calcified nodule in sufferers with acute coronary syndrome by intravascular optical coherence tomography. J Am Coll Cardiol 2013;62:1748–58. https://doi.org/10.1016/j.jacc.2013.05.071
3. O’Donoghue M, Braunwald E, Boden WE et al. Early invasive vs conservative remedy methods in ladies and men with unstable angina and non-ST phase elevation myocardial infarction: a meta-analysis. JAMA 2008;300:71–80. https://doi.org/10.1001/jama.300.1.71
4. Cannon CP, Demopoulos LA, Weintraub WS et al.; TACTICS (Deal with Angina with Aggrastat and Decide Value of Remedy with an Invasive or Conservative Technique) – Thrombolysis in Myocardial Infarction 18 Investigators. Comparability of early invasive and conservative methods in sufferers with unstable coronary syndromes handled with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med 2001;344:1879–87. https://doi.org/10.1056/NEJM200106213442501
5. FRagmin and Quick Revascularisation throughout InStability in Coronary artery illness (FRISC II)Investigators. Invasive in contrast with non-invasive remedy in unstable coronary-artery illness: FRISC II potential randomised multicentre research. Lancet 1999;354:708–15. https://doi.org/10.1016/S0140-6736(99)07349-3
6. Fox KA, Henderson RA, Poole-Wilson PA et al.; Randomized Intervention Trial of unstable Angina Investigators. Interventional versus conservative remedy for sufferers with unstable angina or non-ST-elevation myocardial infarction: the British Coronary heart Basis RITA 3 randomized trial. Lancet 2002;360:743–51. https://doi.org/10.1016/S0140-6736(02)09894-X
7. Nakazawa G, Joner M, Finn AV et al. Delayed arterial therapeutic and elevated late stent thrombosis at perpetrator websites after drug-eluting stent placement for acute myocardial infarction sufferers: an post-mortem research. Circulation 2008;118:1138–45. https://doi.org/10.1161/CIRCULATIONAHA.107.762047
8. Yamamoto M, Okamatsu Ok, Inami S et al. Relationship between neointimal protection of sirolimus-eluting stents and lesion traits: a research with serial coronary angioscopy. Am Coronary heart J 2009;158:99–104. https://doi.org/10.1016/j.ahj.2009.04.016
9. Kramer MC, Rittersma SZ, de Winter RJ et al. Relationship of thrombus therapeutic to underlying plaque morphology in sudden coronary loss of life. J Am Coll Cardiol 2010;55:122–32. https://doi.org/10.1016/j.jacc.2009.09.007
10. Chieffo A, Caussin C, latib A et al. A potential, randomized trial of intravascular-ultrasound guided in comparison with angiography guided stent implantation in advanced coronary lesions: the AVIO trial. Am Coronary heart J 2013;165:65–72. https://doi.org/10.1016/j.ahj.2012.09.017
11. Kang SJ, Park GM, Cho YR et al. Intravascular ultrasound predictors for edge restenosis after newer technology drug-eluting stent implantation. Am J Cardiol 2013;111:1408–14. https://doi.org/10.1016/j.amjcard.2013.01.288
12. Ino Y, Matsuo Y, Kubo T et al. Optical coherence tomography predictors for edge restenosis after everolimus-eluting stent implantation. Circ Cardiovasc Interv 2016;9:e004231. https://doi.org/10.1161/CIRCINTERVENTIONS.116.004231
13. Prati F, Burzotta F, Romagnoli E et al. Medical influence of OCT findings throughout PCI: the CLI-OPCI II research. JACC Cardiovasc Imaging 2015;8:1297–305. https://doi.org/10.1016/j.jcmg.2015.08.013
14. Prati F, Regar E, Mintz GS et al. Knowledgeable overview doc on methodology, terminology, and medical purposes of optical coherence tomography: bodily rules, methodology of picture acquisition, and medical software for evaluation of coronary arteries and atherosclerosis. Eur Coronary heart J 2010;31:401–15. https://doi.org/10.1093/eurheartj/ehp433
15. Witzenbichler B, Weisz G, Maehara A et al. Relationship between intravascular ultrasound steerage and medical outcomes after drug-eluting stents: the Evaluation Of Twin Antiplatelet Remedy with Drug-Eluting Stents (ADAPT-DES) research. Circulation 2014;129:463–70. https://doi.org/10.1161/CIRCULATIONAHA.113.003942
16. Ali ZA, Généreux P, Maehara A et al. Optical coherence tomography in contrast with intravascular ultrasound and with angiography to information coronary stent implantation (ILUMIEN III: OPTIMIZE PCI): a randomized managed trial. Lancet 2016;388:2618–28. https://doi.org/10.1016/S0140-6736(16)31922-5
17. Liu J, Mintz GS, Maehara A et al. An built-in TAXUS IV, V, and VI intravascular ultrasound evaluation of the predictors of edge restenosis after naked steel or paclitaxel-eluting stents. Am J Cardiol 2009;103:501–06. https://doi.org/10.1016/j.amjcard.2008.10.010
18. Prati F, Guagliumi G, Mintz GS et al. Knowledgeable overview doc half 2: methodology, terminology and medical purposes of optical coherence tomography for the evaluation of interventional procedures. Eur Coronary heart J 2012;33:2513–20. https://doi.org/10.1093/eurheartj/ehs095
19. Rezkalla SH, Kloner RA. No-reflow phenomenon. Circulation 2002;105:656–62. https://doi.org/10.1161/hc0502.102867
20. Ramjane Ok, Han L, Jin C. The analysis and remedy of the no-reflow phenomenon in sufferers with myocardial infarction present process percutaneous coronary intervention. Exp Clin Cardiol 2008;13:121–8. Out there from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2586408/
21. Kaivosoja T, Liu S, Dijkstra J et al. Comparability of visible evaluation and pc picture evaluation of intracoronary thrombus kind by optical coherence tomography. PLoS One 2018;13:e0209110. https://doi.org/10.1371/journal.pone.0209110
22. Guagliumi G, Capodanno D, Saia F et al. Mechanisms of atherothrombosis and vascular response to major percutaneous coronary intervention in ladies versus males with acute myocardial infarction: outcomes of the OCTAVIA research. JACC Cardiovasc Interv 2014;7:958–68. https://doi.org/10.1016/j.jcin.2014.05.011
23. Fang C, Dai J, Zhang S et al. Wrongdoer lesion morphology in younger sufferers with ST-segment elevated myocardial infarction: a medical, angiographic and optical coherence tomography research. Atherosclerosis 2019;289:94–100. https://doi.org/10.1016/j.atherosclerosis.2019.08.011
24. Dai J, Xing L, Jia H et al. In vivo predictors of plaque erosion in sufferers with ST-segment elevation myocardial infarction: a medical, angiographical, and intravascular optical coherence tomography research. Eur Coronary heart J 2018;39:2077–85. https://doi.org/10.1093/eurheartj/ehy101
25. Amabile N, Hammas S, Fradi S et al. Intra-coronary thrombus evolution throughout acute coronary syndrome: regression evaluation by serial optical coherence tomography analyses. Eur Coronary heart J Cardiovasc Imaging 2015;16:433–40. https://doi.org/10.1093/ehjci/jeu228
26. Khandkar C, Madhavan MV, Weaver JC et al. Atherothrombosis in acute coronary syndromes – from mechanistic insights to focused therapies. Cells 2021;10:865. https://doi.org/10.3390/cells10040865





























{kind=link}