

The Nationwide Institute for Well being and Care Excellence (NICE) advise towards routine testing for coronary artery illness (CAD) in sufferers with non-anginal chest ache (NACP). This medical audit sought to determine the prevalence of great CAD on this cohort utilizing computed tomography angiography (CTCA) and consider variations within the prevalence of cardiovascular danger components between these with and with out obstructive coronary illness.
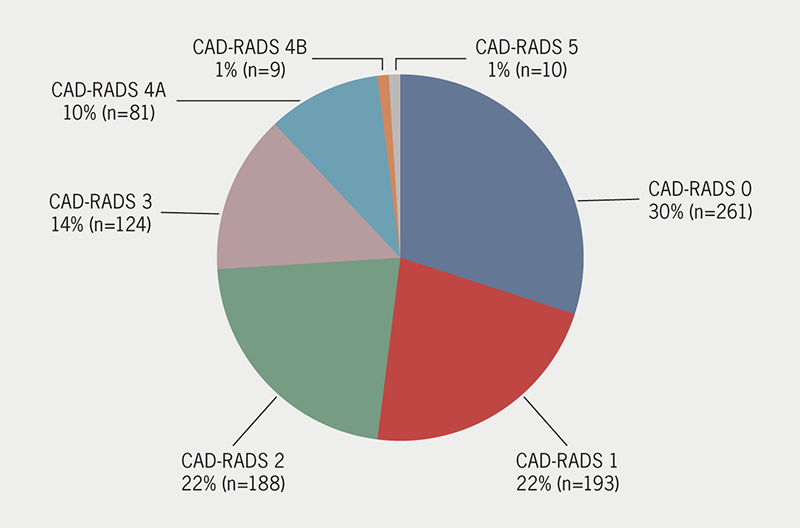
Over 23 months, 866 sufferers with NACP underwent CTCA. Sufferers have been separated into three teams for evaluation relying on the diploma of CAD on CTCA utilizing the CAD-RADS (Coronary Artery Illness Reporting and Information System) scoring system; no proof of CAD (group 1), a level of CAD requiring medical remedy solely (group 2), important CAD outlined as a CAD-RADS rating 4A/B or 5 (group 3). Cardiovascular danger components have been in contrast between the teams.
We discovered 11.5% had important CAD (group 3), 58.3% required medical remedy (group 2) and 30.1% had no CAD (group 1). There have been 32 sufferers who required coronary revascularisation. Sufferers in group 2 and three have been extra more likely to be male (p<0.001) and older (p<0.001) when in comparison with sufferers in group 1. Sufferers in group 3 have been extra more likely to be hypertensive (p=0.008) and have increased Qrisk2 scores (p<0.001) compared with these in group 1.
In conclusion, NICE tips for NACP might lead to a major proportion of sufferers with CAD being underdiagnosed, together with some with extreme illness requiring revascularisation. This evaluation suggests age, male gender, Qrisk2 rating and hypertension are predictors of CAD on this cohort.
Introduction
Coronary artery illness (CAD) is a major reason for morbidity and mortality within the UK, and anginal chest ache is the most typical manifestation.1,2 Chest ache, nevertheless, is without doubt one of the most typical presenting signs in each emergency, main and secondary care, and could be secondary to a myriad of pathologies. Subsequently, the prognosis of CAD from signs alone can show difficult.
Regardless of developments in each invasive and non-invasive CAD imaging, these investigations are usually not with out dangers and price to the well being service. Discount of pointless investigations, whereas figuring out sufferers most in danger, has been a significant motivation behind medical tips. Whereas the newest European and American tips have adopted risk-based methods to determine who to check for CAD,3,4 the Nationwide Institute for Well being and Care Excellence (NICE) medical steerage revealed in 2016 has really useful using affected person signs alone.5 The three key traits of anginal chest ache are: the situation and character of the ache; whether or not or not the ache is precipitated by bodily exertion; and whether or not or not the ache could be relieved inside 5 minutes by relaxation or glyceryl trinitrate spray.5 Sufferers who solely have one among these three key options are mentioned to have non-anginal chest ache (NACP), and the NICE steerage is to desert routine testing for this cohort.
Whereas recognised as a legitimate device for predicting the probability of obstructive CAD,6,7 using signs alone can show troublesome, as sufferers presenting with typical angina solely account for 10–15% of sufferers with CAD.8–10 This may be significantly problematic when assessing feminine sufferers, who usually tend to current with atypical chest ache signs in comparison with males.11 Research recommend that almost all of CAD instances current to cardiology clinics with NACP or atypical angina.10 Moreover, there may be some proof to recommend sufferers presenting with NACP are, the truth is, extra more likely to have underlying CAD than these with atypical angina.9 This, mixed with a bent for clinicians to under-recognise anginal signs, implies that present NICE tips might lead to a major proportion of sufferers with CAD being underdiagnosed, inappropriately reassured, and discharged with out investigations.12
Regardless of the 2016 suggestions, the speedy entry chest ache clinic (RACPC) in our establishment continued to research sufferers with NACP based mostly on a neighborhood cardiac community settlement. Utilizing information from the clinic, this medical audit aimed to determine the prevalence of obstructive CAD on this cohort, and search for predictive markers which may assist to danger stratify such sufferers sooner or later.
Supplies and technique
Between 1 January 2017 and 1 December 2019, 1,034 sufferers with no prior historical past of ischaemic coronary heart illness offered to the RACPC with one of many three key options of typical angina (and have been, subsequently, deemed to have NACP), and have been referred for computed tomography coronary angiography (CTCA). Sufferers that have been unable to have CTCA as a consequence of poor renal or lung perform have been as an alternative referred for stress echocardiography and have been excluded from the evaluation. All sufferers attending the clinic acquired data sheets explaining their anonymised information could also be used for service analysis and medical audit. Because the evaluation was deemed to be a medical audit, moral approval from the belief’s native ethics committee was not required.
Sufferers have been recognized utilizing the clinic database, and the belief’s digital report system and imaging database have been used to analyse CTCA outcomes. Throughout clinic triage, the incidence of cardiovascular danger components was recorded and documented within the clinic database for every affected person. These danger components included age, gender, diabetes, hypertension, household historical past of heart problems and hypercholesterolaemia. The Qrisk2 rating was additionally calculated for all sufferers.13
All sufferers have been referred for a CTCA as a first-line non-invasive investigation for CAD, and their photos have been learn by professional readers. The CAD-RADS (Coronary Artery Illness Reporting and Information System) scoring system was used to determine the diploma of luminal stenosis and the coronary calcium rating (Agatston/quantity) was used to determine the calcium burden on CTCA.14 For the aim of this evaluation, sufferers have been divided into three teams based on the diploma of CAD on CTCA:
Group 1 (no proof of CAD): CAD-RADS rating 0
Group 2 (diploma of CAD requiring medical preventative remedy solely): CAD-RADS rating 1–3
Group 3 (important CAD): CAD-RADS 4A/4B or 5.
Inside group 2, the variety of sufferers with a Qrisk2 rating of lower than 10% was additionally calculated, as this cohort wouldn’t have been eligible for a main prevention statin previous to investigations, based on NICE tips.15 Sufferers with a CAD-RADS rating of three, or extreme calcification on CTCA, are deemed excessive danger and sometimes endure additional testing for CAD. Subsequently, together with these in group 3, the data of sufferers in group 2 or with extreme calcification on CTCA, have been additionally analysed to determine people who underwent invasive angiography and revascularisation procedures.
The prevalence of the aforementioned cardiovascular danger components have been in contrast between every group. The ANOVA take a look at was used to match age, the Kruskal-Wallis take a look at to match Qrisk2 scores and the Chi-squared take a look at to match gender and the prevalence of diabetes, hypertension, household historical past and hypercholesterolaemia between the teams. The place important variations between teams have been discovered, post-hoc evaluation was used to account for any false discovery. The place important variations have been discovered between the teams, 95% confidence intervals (CI) have been calculated.
Outcomes
Desk 1. Causes for sufferers not having luminal evaluation on computed tomography coronary angiography (CTCA)
Causes for non-interpretable CTCA
No. of sufferers
Extreme calcification
111
Tachycardia
34
Poor picture or movement artefact
12
Distinction allergy or uncomfortable side effects
4
Non-attendance or refused scan
4
Atrial fibrillation
3
In complete, 1,034 sufferers attended the clinic with NACP and have been referred for a CTCA. 4 sufferers refused to have the scan or didn’t attend, and 4 sufferers have been unable to have the scan as a consequence of earlier distinction allergy symptoms or uncomfortable side effects. Of the 1,026 sufferers who proceeded with a CTCA, 160 sufferers have been unable to have luminal evaluation as a consequence of extreme calcification, gating difficulties (as a consequence of tachycardia or atrial fibrillation) and poor photos or movement artefacts (see desk 1 for breakdown).
In complete, 866 sufferers (51.4% male, 48.6% feminine) had a CTCA that allowed luminal evaluation and calcium scoring. We discovered that 30.1% (n=261) of sufferers met the factors for group 1 and had no proof of CAD on their CTCA. An additional 58.3% (n=505) of sufferers had a CAD-RADS rating of 1–3 and required medical preventative remedy. Inside this group, 32.5% (n=164) had a Qrisk2 rating of lower than 10%. In complete, 11.5% (n=100) of sufferers met the factors for group 3 and had proof of great CAD on CTCA. The CAD-RADS scores for these sufferers could be seen in determine 1. 9 sufferers from group 2, 37 sufferers from group 3, and 12 sufferers with extreme calcification on CTCA underwent invasive angiography following their CTCA so as to add readability to the prognosis. In group 2, two sufferers underwent revascularisation procedures (one had a percutaneous coronary intervention [PCI] and one had a coronary artery bypass graft [CABG]). Six sufferers with extreme calcification on their preliminary CTCA underwent revascularisation (two PCI and 4 CABG). In group 3, 24 sufferers underwent revascularisation procedures (19 PCI and 5 CABG).
As regards to cardiovascular danger components, evaluation revealed that sufferers in both group 2 or group 3 have been extra more likely to be older than sufferers in group 1 (group 1 55.6 ± 10.3 years vs. group 2 60 ± 9.9 years, p<0.001; vs. group 3 62.3 ± 9.3 years, p<0.001). Moreover, sufferers in group 2 and group 3 have been extra more likely to be male in comparison with these in group 1 (55% in group 2 vs 40% in group 1, p<0.001; 62% in group 3 vs 40% in group 1, p<0.001). Sufferers with important CAD have been additionally extra more likely to be hypertensive than sufferers with no CAD on CTCA (28% in group 1 vs. 45% in group 3, p=0.008). Moreover, important variations in Qrisk2 scores have been discovered between all three teams (determine 2). Sufferers in group 3 had a imply Qrisk2 rating of 19.5 (interquartile vary [IQR] 12.4–27), in contrast with 13.5 (IQR 8.3–20.4) in group 2 and 9.1 (IQR 6.4–14.9) in group 1. The variations in Qrisk2 scores between all three teams have been important at p<0.001. Though sufferers in group 3 have been extra more likely to be diabetic and have a household historical past of heart problems compared with the these in group 1 and a couple of, this was not statistically important (p=0.217 and p=0.314, respectively). No important distinction within the prevalence of hypercholesterolaemia was discovered between the three teams (desk 2).

Desk 2. A comparability of the prevalence of cardiovascular danger components between the three teams
Variables
All sufferers (n=866)
Group one (n=261)
Group two (n=505)
Group three (n=100)
Take a look at
p worth
Submit-hoc take a look at
Variations between teams
Imply age ± SD, years
58.9 ± 10.2
55.6 ± 10.3
60 ± 9.9
62.3 ± 9.3
ANOVA
<0.001
Tukey HSD
Group 1 considerably totally different to teams 2 and three
Male gender, n (%)
445 (51)
105 (40)
278 (55)
62 (62)
Chi-squared
<0.001
Prop take a look at
Group 1 considerably totally different to teams 2 and three
Qrisk2, median (IQR)
12.7 (7.7–20.5)
9.1 (6.4–14.9)
13.5 (8.3–20.4)
19.5 (12.4–27)
Kruskal-Wallis
<0.001
Pair-wise Wilcoxon rank sum
All teams considerably totally different
Diabetes, n (%)
117 (14)
36 (14)
61 (12)
20 (20)
Chi-squared
0.217
Hypertension, n (%)
293 (34)
73 (28)
175 (35)
45 (45)
Chi-squared
0.008
Prop take a look at
Group 1 considerably totally different to group 3
Household historical past, n (%)
354 (41)
105 (40)
202 (40)
47 (47)
Chi-squared
0.314
Hypercholes-terolaemia, n (%)
144 (17)
39 (15)
91 (18)
14 (14)
Chi-squared
0.856
Key: ANOVA = evaluation of variance; HSD = actually important distinction; IQR = interquartile vary; SD = normal deviation
Dialogue
This evaluation of sufferers presenting with NACP in a area of excessive inhabitants prevalence of CAD, confirmed that almost two-thirds had some extent of coronary atheroma on CTCA. Certainly, 11.5% of sufferers had obstructive CAD on CTCA, with round 1 / 4 of those sufferers having prognostic illness warranting revascularisation procedures. An additional 58.3% had a level of CAD warranting medical remedy with statins. Of those sufferers, 32.5% had a Qrisk2 rating of lower than 10% and, subsequently, wouldn’t have certified for a main prevention statin previous to their CTCA, based on NICE tips. Sufferers with a CAD-RADS rating of three at our establishment went on to have purposeful testing, nevertheless, this audit didn’t seize these discovered to have ischaemia on these assessments. This, together with our exclusion of sufferers with excessive calcium scores prohibiting luminal evaluation, means the prevalence of great CAD could also be even increased on this cohort. Our medical audit means that adhering to present NICE tips ends in a major proportion of sufferers with CAD being underdiagnosed and wrongly reassured.
The prevalence of extreme CAD on this medical audit is just like different databases. Information from the worldwide, multi-centre CONFIRM (Coronary CT Angiography Analysis for Medical Outcomes: An Worldwide Multicenter) registry revealed that 11.7% of 1,253 sufferers with NACP present process clinically indicated CTCA had >70% luminal stenosis.9 Of their database, the precise prevalence of >50% luminal stenosis was the truth is decrease than guideline prediction for many sufferers presenting with chest ache. The one exception was the NACP cohort who, the truth is, had increased than predicted average CAD on angiography. Within the American School of Cardiology registry, sufferers with atypical angina had the bottom prevalence of CAD of all of the teams, together with these with NACP and no chest ache.16 In addition to this, there may be proof that NACP is related to important morbidity and mortality if left untreated. Of their five-year evaluation of sufferers attending RACPCs throughout a number of centres in England, Sekhri et al. discovered that sufferers identified with NACP accounted for round a 3rd of sufferers that suffered both acute coronary syndrome or died from heart problems throughout follow-up.17 This means that NICE steerage proposing investigations for sufferers with atypical angina, and never for these with NACP, could also be a missed alternative.
With all steerage for suspected angina, there’s a stability to be struck between the widespread use of a expertise with a unfavourable yield, but figuring out the sufferers at highest danger of needing revascularisation. If the aim of the NICE steerage is to diagnose sufferers with obstructive CAD, then information from the CONFIRM and American registries recommend that the one group that must be investigated with anatomical testing is these with typical angina, as that is the one symptom group that strongly predicted important obstructive illness on CTCA.9,16 Nonetheless, of their post-hoc evaluation of the 2015 SCOT-HEART (Scottish Computed Tomography of the Coronary heart) examine dataset,18 Adamson et al. discovered that CTCA imaging resulted in a rise within the charges of invasive angiography in sufferers with NACP, with no improve within the pick-up of obstructive illness and revascularisation procedures, thereby, supporting using NICE tips.19 Nonetheless, CTCA nonetheless recognized obstructive illness in 9.5% of sufferers with NACP, with 2.2% of sufferers present process revascularisation procedures and 19.4% having therapy adjustments. Within the preliminary 2015 SCOT-HEART examine, the improved outcomes in sufferers present process CTCA versus normal care have been achieved by way of preventative therapies quite than revascularisation,18 highlighting the significance of optimising medical remedy on this cohort. In our evaluation, 18.9% of sufferers with NACP wouldn’t have benefited from acceptable preventative remedy beneath the present NICE steerage.
We do, nevertheless, acknowledge that the blanket use of imaging in all sufferers with NACP will not be with out its disadvantages. The plain difficulties embody value, in addition to the manpower to carry out and interpret imaging. Though there may be growing proof to recommend CTCA is a cheap strategy to determine CAD in sufferers with low-to-intermediate danger of illness, only a few research embody the ‘no-testing’ strategy proposed by NICE.20 Moreover, even when important CAD is detected on anatomical imaging, there may be little proof to recommend that revascularisation of sufferers with steady CAD improves outcomes.21 This will likely recommend that, until sufferers are restricted by their angina signs and refractory to medical remedy, an elevated detection of great CAD on imaging might result in pointless and high-risk procedures.22
In conclusion, this medical audit means that present NICE tips for the investigation of sufferers with NACP might result in the underdiagnosis of great illness, particularly in excessive prevalence areas of the UK.1 This evaluation discovered that almost two-thirds of the sufferers attending our centre had CAD even with chest ache that was categorised as non-anginal. Qrisk2 rating, male gender, age and a historical past of hypertension have been the strongest predictors of CAD on this cohort. Whereas RACPCs are usually not meant for inhabitants screening for CAD, our findings recommend {that a} extra nuanced use of the NICE tips must be thought of, particularly in excessive prevalence areas.
Key messages
Present Nationwide Institute for Well being and Care Excellence (NICE) tips advise towards routine testing for coronary artery illness (CAD) in sufferers presenting with non-anginal chest ache (NACP)
Practically two-thirds of sufferers attending a speedy entry chest ache clinic with NACP had a level of CAD on computed tomography coronary angiography (CTCA). A complete of 11.5% of sufferers had important CAD on CTCA, with round 1 / 4 of those sufferers requiring revascularisation procedures
Qrisk2 rating, age, male gender and a historical past of hypertension have been predictors of CAD on this cohort
Our findings recommend {that a} extra nuanced use of the NICE tips for NACP must be thought of, particularly in excessive prevalence areas
Conflicts of curiosity
None declared.
Funding
None.
Examine approval
All sufferers attending the clinic acquired data sheets explaining their anonymised information could also be used for service analysis and medical audit. Because the evaluation was deemed to be a medical audit, moral approval from the belief’s native ethics committee was not required.
References
1. British Coronary heart Basis. UK Factsheet January 2022. London: BHF, 2022. Out there from: https://www.bhf.org.uk/what-we-do/our-research/heart-statistics [accessed 25 November 2022].
2. Kannel WB, Feinleib M. Pure historical past of angina pectoris within the Framingham examine. Prognosis and survival. Am J Cardiol 1972;29:154–63. https://doi.org/10.1016/0002-9149(72)90624-8
3. Activity Drive Members, Montalescot G, Sechtem U et al. 2013 ESC tips on the administration of steady coronary artery illness: the Activity Drive on the administration of steady coronary artery illness of the European Society of Cardiology. Eur Coronary heart J 2013;34:2949–3003. https://doi.org/10.1093/eurheartj/eht296
4. Gibbons RJ, Chatterjee Ok, Daley J et al. ACC/AHA/ACP-ASIM tips for the administration of sufferers with persistent steady angina: govt abstract and proposals. Circulation 1999;99:2829–48. https://doi.org/10.1161/01.CIR.99.21.2829
5. Nationwide Institute for Well being and Care Excellence. Latest-onset chest ache of suspected cardiac origin: evaluation and prognosis. CG95. London: NICE, 2016. Out there from: https://www.good.org.uk/steerage/cg95/chapter/Suggestions
6. Diamond G. A clinically related classification of chest discomfort. J Am Coll Cardiol 1983;1:574–5. https://doi.org/10.1016/S0735-1097(83)80093-X
7. Genders TS, Steyerberg EW, Hunink MG et al. Prediction mannequin to estimate presence of coronary artery illness: retrospective pooled evaluation of present cohort. BMJ 2012;344:e3485. https://doi.org/10.1136/bmj.e3485
8. Reeh J, Therming CB, Heitmann M et al. Prediction of coronary artery illness and prognosis in sufferers with suspected steady angina. Eur Coronary heart J 2018;40:1426–35. https://doi.org/10.1093/eurheartj/ehy806
9. Cheng VY, Berman DS, Rozanski A et al. Efficiency of the normal age, intercourse, and angina typicality-based strategy for estimating pretest likelihood of angiographically important coronary artery illness in sufferers present process coronary computed tomographic angiography: outcomes from the multinational coronary CT angiography analysis for medical outcomes: a world multicenter registry (CONFIRM). Circulation 2011;124:2423–32. https://doi.org/10.1161/CIRCULATIONAHA.111.039255
10. Douglas PS, Hoffmann U, Patel MR et al. Outcomes of anatomical versus purposeful testing for coronary artery illness. N Engl J Med 2015;372:1291–300. https://doi.org/10.1056/NEJMoa1415516
11. Sharma SP, Manintveld OC, Buddle R et al. Gender Variations in Sufferers With Secure Chest Ache. Am J Cardiol 2022;171:84–90. https://doi.org/10.1016/j.amjcard.2022.01.054
12. Arnold SV, Grodzinsky A, Gosch KL et al. Predictors of doctor under-recognition of angina in outpatients with steady coronary artery illness. Circ Cardiovasc Qual Outcomes 2016;9:554–9. https://doi.org/10.1161/CIRCOUTCOMES.116.002781
13. Collins GS, Altman DG. An impartial and exterior validation of QRISK2 heart problems danger rating: a potential open cohort examine. BMJ 2010;340:c2442. https://doi.org/10.1136/bmj.c2442
14. Cury RC, Abbara S, Achenbach S et al. CAD-RADS™: Coronary Artery Illness – Reporting and Information System: an professional consensus doc of the Society of Cardiovascular Computed Tomography (SCCT), the American School of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American School of Cardiology. J Am Coll Radiol 2016;13(12 Pt A):1458.e9–1466.e9. https://doi.org/10.1016/j.jacr.2016.04.024
15. Nationwide Institute for Well being and Care Excellence. Cardiovascular danger evaluation and lipid modification. QS100. London: NICE, 2015. Out there from: https://www.good.org.uk/steerage/qs100/chapter/quality-statement-5-statins-for-primary-prevention
16. Patel MR, Peterson ED, Dai D et al. Low diagnostic yield of elective coronary angiography. N Engl J Med 2014;362:886–95. https://doi.org/10.1056/NEJMoa0907272
17. Sekhri N, Feder GS, Junghans C et al. How efficient are speedy entry chest ache clinics? Prognosis of incident angina and non-cardiac chest ache in 8762 consecutive sufferers. Coronary heart 2007;93:458–63. https://doi.org/10.1136/hrt.2006.090894
18. SCOT-HEART investigators. CT coronary angiography in sufferers with suspected angina as a consequence of coronary coronary heart illness (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet 2015;385:2383–91. https://doi.org/10.1016/S0140-6736(15)60291-4
19. Adamson PD, Hunter A, Williams MC. Diagnostic and prognostic advantages of computed tomography coronary angiography utilizing the 2016 Nationwide Institute for Well being and Care Excellence steerage inside a randomised trial. Coronary heart 2018;104:207–14. https://doi.org/10.1136/heartjnl-2017-311508
20. van Waardhuizen CN, Khanji MY, Genders TS et al. Comparative cost-effectiveness of non-invasive imaging assessments in sufferers presenting with persistent steady chest ache with suspected coronary artery illness: a scientific overview. Eur Coronary heart J Qual Care Clin Outcomes 2016;2:245–60. https://doi.org/10.1093/ehjqcco/qcw029
21. Lin GA, Dudley RA. Combating the “oculostenotic reflex”. JAMA Intern Med 2014;174:1621–2. https://doi.org/10.1001/jamainternmed.2014.164
22. Maron DJ, Hochman JS, Reynolds HR et al. Preliminary invasive or conservative technique for steady coronary illness. N Engl J Med 2020;382:1395–407. https://doi.org/10.1056/NEJMoa1915922




























{kind=link}